When Pain Science Caught Up
How Black healers and physicians shaped the way we treat pain today
Anya Griffin, PhD
Babies & Toddlers (0-2) Kids (3-11) Tweens & Teens (12+) Healthcare Providers Acute Pain Chronic Pain Procedural Pain English
Share this:
Pain is universal, but the science of how we treat it has been shaped by those who were forced to innovate in the face of exclusion. This Black History Month 2026, we honor the Black healers, physicians, and researchers who didn’t just join the medical field—they revolutionized it. From ancestral indigenous practices with plant medicines to modern trauma-informed care, the foundation of how we understand pain today is rooted in the contributions of Black Medicine.
Pain Care Born in Community: The First Integrated Medicine
For much of U.S. history, systemic exclusion meant Black communities had to develop their own specialized pain management. Long before modern neuroscience coined the term “nervous-system regulation,” Black midwives and community healers were practicing it.
They understood that pain is amplified by fear and isolation. By using plant medicines, warmth, and “laying of hands,” they created an environment of safety and healing. We now know that when the nervous system feels safe, the brain reduces pain signaling. These healers weren’t just providing comfort; they were practicing early biopsychosocial medicine.
Today’s leading pain programs follow the biopsychosocial model, recognizing that pain is influenced not only by injury and inflammation but also by the nervous system, emotions, stress, and social connection.
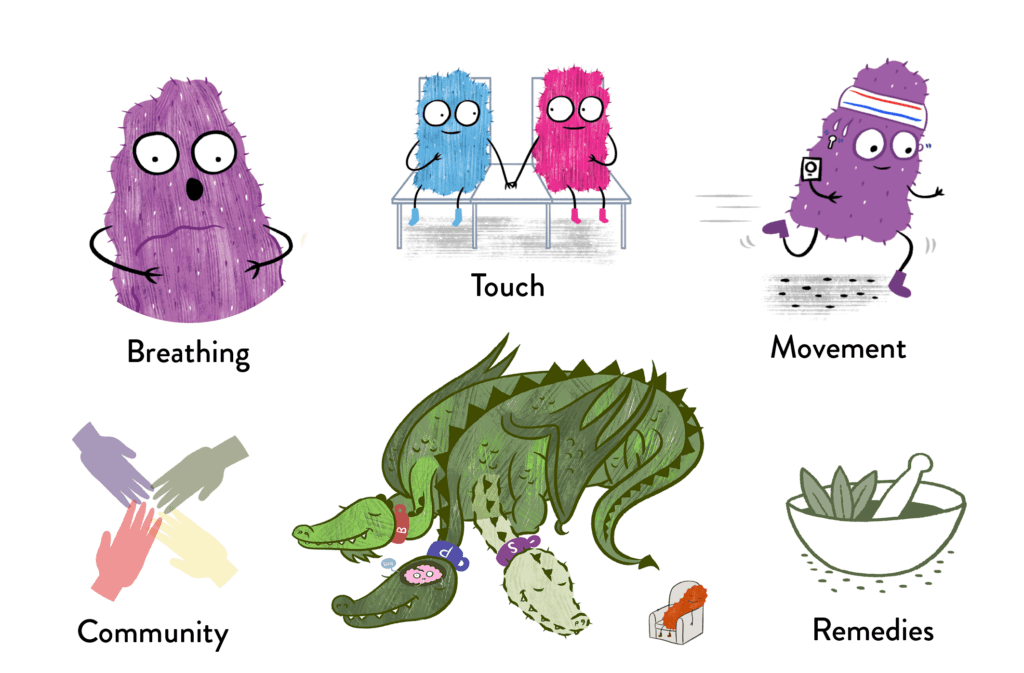
This framework closely mirrors Black healing traditions:
- Breathing and calming practices that regulate stress responses
- Movement and physical effort to restore function
- Touch, warmth, and reassurance to signal safety
- Family and community involvement as part of healing
- Plant-based and integrative remedies for inflammation and discomfort
Modern treatments—breathing techniques, physical therapy, biofeedback, psychological therapies, and family-based care—are not separate from medicine. They are scientifically validated extensions of healing traditions that Black communities preserved when formal care was unavailable or unsafe. In many ways, modern pain science has caught up to what Black healers already knew.
The Correctors: Physicians Who Dismantled Myths
Black physicians used scientific rigor to dismantle dangerous medical myths that still impact patients today.
Dr. James McCune Smith: The first Black American to earn a medical degree, he used data to destroy racist theories about biological differences in pain tolerance. His work remains the blueprint for Health Equity Scorecards used today to monitor treatment fairness.

Dr. Rebecca Lee Crumpler: Her 1883 Book of Medical Discourses was a pioneer in pediatric care, emphasizing that a child’s discomfort cannot be separated from their home and emotional environment.
Dr. Charles Drew: By revolutionizing blood banking, he transformed surgical recovery, making aggressive pain management possible for trauma survivors worldwide.
Transforming Crisis into Care: The Sickle Cell Legacy
One of the most profound shifts in pain medicine came from Black clinicians advocating for patients diagnosed with Sickle Cell Disease (SCD). Previously dismissed or misunderstood, these pioneers proved that SCD pain crises are:
- Biological Emergencies: Requiring rapid, high-level intervention.
- Neurological Events: Capable of “sensitizing” the nervous system, leading to chronic pain.
Because of this important work, today we have emergency protocols that now prioritize “rapid-access” pain relief, ensuring that patient reports of pain are treated as objective medical facts.
A Living Legacy
Modern pain science hasn’t just evolved; it has “caught up” to what Black healers and physicians have known for centuries: healing requires the whole person. Whether it’s through breathing techniques, exercises taught in physical therapy, or the rapid administration of analgesics in an ER, the influence of Black medicine is present in every act of compassionate care. This month, we don’t just look back at what Black medicine endured—we look at the high standard of care it built for everyone.
Advocacy: A Toolkit for Families
While the legacy is strong, disparities in pediatric pain management persist. Families can honor this history by being their child’s fiercest advocate using these modern tools:
Standardize the Assessment: Use the Wong-Baker FACES Scale during appointments to provide a visual, objective score that reduces the chance of provider bias.
Shared Decision-Making: Requesting opportunities for shared medical decision-making can help ensure a child’s needs are being met. For example, use the phrase: “Can we walk through all the options, both medicinal and integrative care, to ensure my child has optimal pain reduction?”
The “Second Voice”: Today, many hospitals offer Patient Advocates. If you feel your child’s pain is being downplayed or undertreated, ask to speak with a Patient Liaison or a Child Life Specialist immediately.
Document the Narrative: Keep a “Pain Diary” that tracks sleep, mood, and activity levels. Hard data is a powerful tool against implicit bias.
Pain is universal. And the science we use to treat it was built by Black healers, physicians, and researchers. Every time a provider treats the whole child, not just the symptom, that legacy is alive in the room.
You May Also Be Interest In

Blog Post
Racial disparities in pain management: How the color of your skin can determine what kind of care you get
Racial bias impacts every aspect of healthcare, including pain treatment. Pretending otherwise perpetuates a system that creates needless suffering. It's time we do better.

Blog Post
"But You Look Fine…": Gender Bias And Pain Care
Dr. Grace Kao's personal account (backed by powerful research) highlights how gender and bias play out when it comes to treating women's pain.

Blog Post
Pain Management for Trans and Gender Diverse Youth
At Meg Foundation, we’re all about empowering children and families with resources that will help them be more comfortable and less anxious during medical procedures. For trans and gender diverse youth, the word “empowerment” is a critical part of their medical vocabulary.
Blog Post
5 Ways Pain Affects the LGBTQIA+ Community
Pain isn’t just physical—it’s deeply shaped by who we are, how we see ourselves, and how the world treats us. For LGBTQIA+ individuals, understanding and addressing pain means recognizing the powerful role of identity, community, and inclusive, affirming care.

About the Author
Dr. Anya Griffin is a pediatric psychologist and Director of Psychology at Children’s Hospital Los Angeles. Dr. Griffin brings over a decade of experience working with children and adolescents facing complex medical conditions, including chronic pain, cancer, and sickle cell disease.
A licensed clinical psychologist and board-certified dance/movement therapist, Dr. Griffin earned her master’s degree in Dance/Movement Therapy from UCLA and her PhD in Clinical Psychology with a specialization in Health Psychology from Fielding Graduate University. She completed her clinical training at Children’s Hospital Los Angeles and Children’s Healthcare of Atlanta. Her work focuses on integrating mind-body strategies into pediatric pain care, supporting smooth transitions from pediatric to adult healthcare, and using creative approaches like photographic storytelling to amplify patient voices.